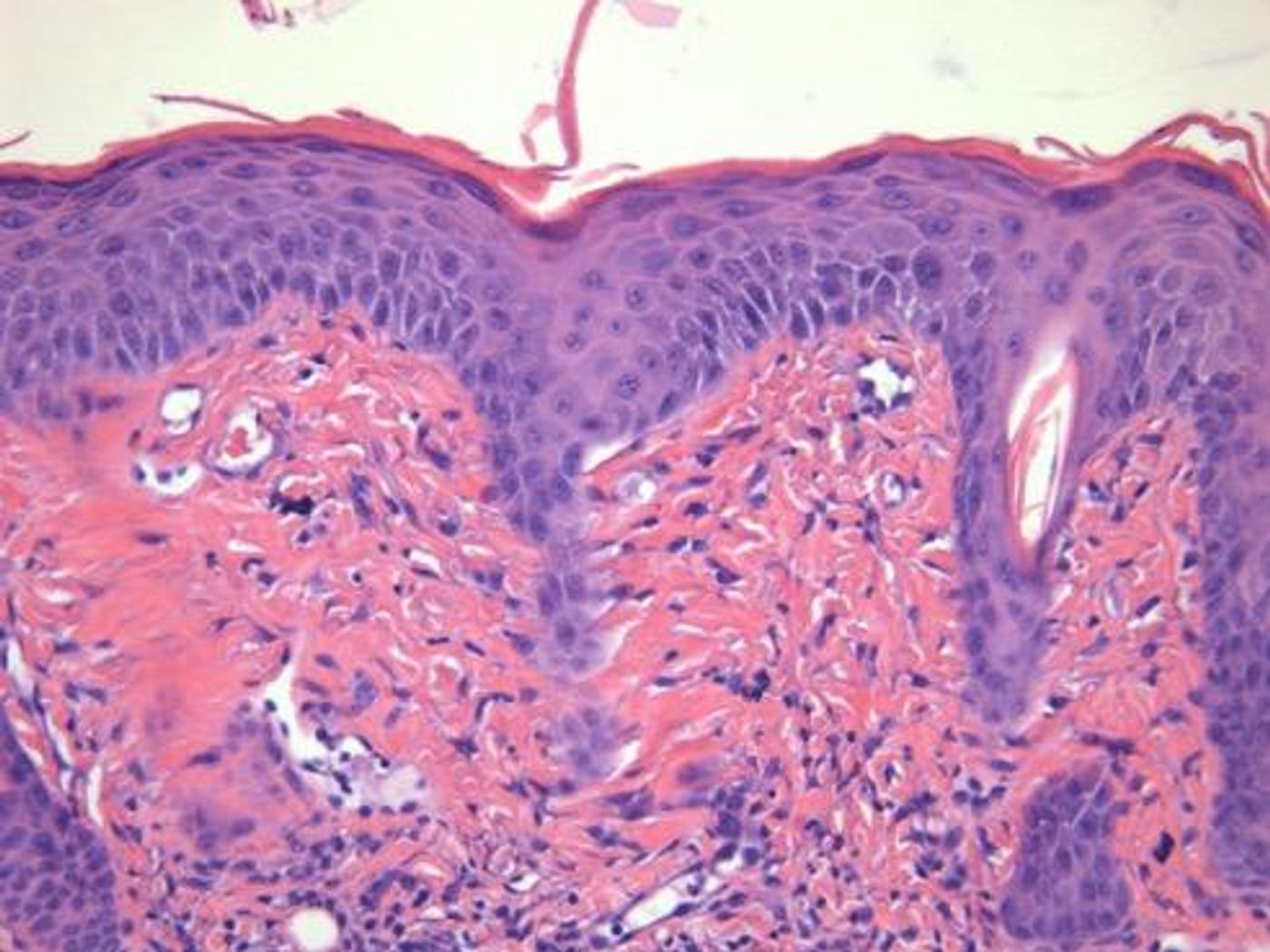
Psoriasis is an autoimmune disease that primarily affects the skin, but individuals with this disease are at a significantly increased risk of heart disease. How are the two systems connected? In a new study from Case Western Reserve University, researchers identified and studied the inflammatory molecules that tie the two conditions together, in hopes for developing a treatment to simultaneously treat psoriasis and prevent adverse cardiac events.
With 1 in 50 people living with psoriasis worldwide, scientists are very invested in understanding and preventing comorbidities associated with the disease. For psoriasis patients at an increased risk of heart attacks and stroke from artery inflammation all over the body, researchers like Case Western Reserve University’s Nicole Ward, PhD, are dedicated to understanding the molecular connection, which increases an individual’s risk of thrombosis, including fatal blood clots.
Ward and her team first looked at interleukin-6 (IL-6), one type of chemical messenger incorporated by the immune system to trigger different inflammatory of anti-inflammatory pathways. In an autoimmune disease like psoriasis, it was no surprise when researchers noticed high levels of IL-6 in the skin of patients. They quickly made the connection between psoriasis and heart disease here because many patients with congestive heart failure also show signs of elevated IL-6.
In the case of psoriasis, IL-6 stimulates excessive inflammation that causes the characteristic overproduction of skin cells present in psoriasis patients. However, similar inflammation triggered by IL-6 but present in the arteries could also be causing heart disease.
However, studies in mouse models showed that removing IL-6 reduced cardiovascular risk but could not treat psoriasis successfully on its own. "Eliminating this one molecule just isn't good enough,” Ward said.
So if it’s not IL-6, what is the connection between the two conditions? The next suspect was a protein called MRP14, which is reliably used by scientists to predict the risk of heart attack in certain groups of people. Psoriasis patients also have high levels of MRP14 in their blood, and the gene coding for MRP14 is relatively near to the genes coding for psoriasis characteristics. MRP14 was the logical next piece of the puzzle. Could the protein be playing a role in both disease pathways?
Again, they tested in mice by knocking out the gene coding for MRP14, but researchers so no effect on skin inflammation or heart disease. "The MRP14-deficient psoriasis mice were completely the same as the regular psoriasis mice,” Ward said. “They all had similar levels of skin inflammation and thrombosis."
At this point Ward and her team knew that the culprit was neither IL-6 nor MRP14, at least not individually. There had to be another component involved, someone to drive the getaway car.
Without MRP14, mice models of psoriasis still showed high levels of IL-6 in addition to two other pro-inflammatory molecules: IL-23 and IL-17. This observation led Ward to believe that these two molecules were “helping” compensate for a lack of MRP14 in the system, making up for the loss of inflammatory molecules and maintaining the same level of skin inflammation that would occur if MRP14 were present.
Meanwhile, these two molecules were already severely under the spotlight via scientists studying and developing the newest treatments for psoriasis. "We discovered that blocking IL-23/IL-17 decreased skin-derived IL-6 in MRP14-deficient psoriasis mice and reversed the thrombosis,” Ward said, describing the type of result she had anticipated from the studies blocking IL-6 and MRP14.
Ward then set out to identify more immune molecules influenced by the genetic deletion of IL-6 in psoriasis mice models. “It is possible that these factors also increase in psoriasis patient skin and explain why they do not respond clinically to IL-6 blockade,” Ward explained.
At first glance, the results from the first part of the study where researchers blocked the expression of IL-6 showed that although the molecule seemed to be connected to both psoriasis and its cardiac comorbidities, inhibiting the molecule would not lead to any therapeutic results. But with Ward’s study, researchers now understand both the similarities and the differences between the psoriasis and thrombosis pathways that intricately define how and when psoriasis patients experience and increased risk of heart disease.
"You have to dig deep and find something interesting from the experiments that don't work out the way you want them to,” Ward said. She and her team will continue to research IL-6, focusing on its interaction with blood and the vessel wall in relation to thrombosis.
Altogether Ward’s research was published in two different articles from the
Journal of Clinical Investigation Insight and the
Journal of Investigative Dermatology.
Sources:
Case Western Reserve University,
National Psoriasis Foundation