A new 3D virtual heart may help doctors identify which cardiac patients are most at risk for life-threatening arrhythmia and need a defibrillator to keep their heartbeats steady and strong.
The computer model, customized for individual patients, could eventually replace the imprecise blood pumping measurement doctors now use to decide whether to put their patients through invasive surgery to place a defibrillator in the chest or abdomen.
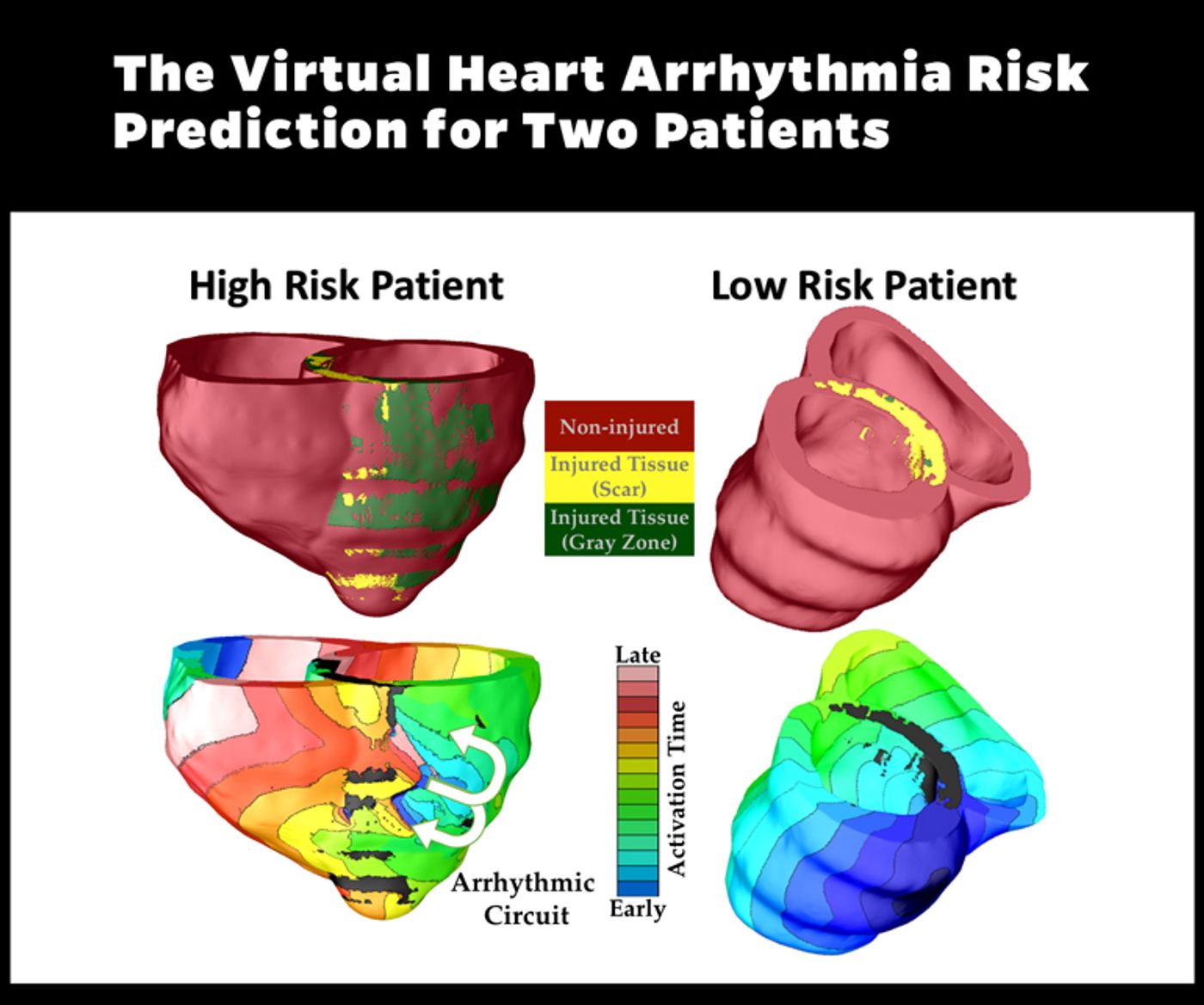
Full graphic and caption from above is available
here.
In a proof-of-concept report in the journal
Nature Communications, researchers report that the new digital approach yielded more accurate predictions of arrhythmia risk than the traditional ejection fraction assessment.
“Our virtual heart test significantly outperformed several existing clinical metrics in predicting future arrhythmic events,” says Natalia Trayanova, professor of biomedical engineering at Johns Hopkins University. “This non-invasive and personalized virtual heart-risk assessment could help prevent sudden cardiac deaths and allow patients who are not at risk to avoid unnecessary defibrillator implantations.”
Arrhythmia is an irregular heartbeat—too fast or too slow—that occurs when electrical waves that govern the heart’s beating pattern run amok. It may be triggered or worsened by heart damage; it can be relatively harmless or life-threatening. A defibrillator can sense the onset of arrhythmia and administer an electric shock to jolt the heart back to a normal rhythm.
The researchers used MRI records of patients who had survived a heart attack but were left with damaged cardiac tissue. The 41 patients each had an ejection fraction—a measure of how much blood is being pumped out of the heart—of less than 35 percent and so each had had a defibrillator implant. While building each patient’s custom 3D virtual heart to assess his or her arrhythmia risk, the researchers did not know whether that patient had experienced arrhythmia in real life.
Using computer-modeling techniques developed in Trayanova’s lab, a replica of each patient’s heart was brought to life with representations of the electrical processes in the cardiac cells and communication among cells. In some cases, the virtual heart developed an arrhythmia, and in others it did not. The result was dubbed VARP, short for virtual-heart arrhythmia risk predictor. The method accounts for the geometry of the patient’s heart, the way electrical waves move through it, and the impact of scar tissue left by the earlier heart attack.
Eventually, VARP results were compared to patients’ real-life post-implantation records to see how well the technology predicted which patients would experience arrhythmias. Patients found by VARP to be at-risk were four times more likely to have had arrhythmia than those who tested negative. VARP predicted arrhythmia occurrence four-to-five times better than ejection fraction and other existing risk predictors.
“We demonstrated that VARP is better than any other arrhythmia prediction method that is out there,” Trayanova says. “By accurately predicting which patients are at risk of sudden cardiac death, the VARP approach will provide the doctors with a tool to identify those patients who truly need the costly implantable device, and those for whom the device would not provide any life-saving benefits.”
Encouraging early results indicate that the more nuanced, individualized VARP technique could be a useful alternative to the one-size-fits-all ejection fraction score, says cardiologist Katherine C. Wu, associate professor at the Johns Hopkins School of Medicine. “This represents a safer, more comprehensive and individualized approach to sudden cardiac death risk assessment.”
An implantable defibrillator carries risks of its own; avoiding implantation when one is not needed eliminates these risks. Implantable defibrillators require invasive access to the heart, frequent checks and intermittent battery changes. Complications can include infection, malfunction and, in rare instances, heart or blood vessel damage.
With the proof-of-concept study completed, the researchers hope to conduct tests with larger groups of heart patients. The VARP technique is covered by patent protection.
The National Institutes of Health, American Heart Association, and W.W. Smith Charitable Trust funded the work.
Source:
Johns Hopkins University
This article was originally published on
futurity.org.