 Molecular Respiratory Panels — Importance of Differential Diagnosis
Molecular Respiratory Panels — Importance of Differential Diagnosis
With Respiratory Season rapidly approaching the Northern Hemisphere, clinical laboratories must consider diagnostic strategies that produce maximum clinical utility, utilize efficient workflows, and minimize costs. Respiratory tract infections remain among the most common causes of morbidity worldwide, accounting for a significant proportion of outpatient visits, emergency care utilization, and hospital admissions. The etiologies are diverse, ranging from influenza and respiratory syncytial virus (RSV) to rhinovirus and atypical organisms. Clinical presentation alone is often insufficient for definitive diagnosis, as overlapping symptoms—fever, cough, sore throat, nasal congestion, and malaise—can result from multiple viral or bacterial agents. In this context, molecular respiratory panels have emerged as critical tools guiding clinical decision-making and laboratory efficiency.
Advantages of Molecular Respiratory Panels
Unlike traditional culture or antigen-based methods, molecular assays provide:
- High sensitivity and specificity for a wide range of viral targets.
- Rapid turnaround time, supporting timely infection control measures and appropriate therapy.
- Multiplex capacity, allowing simultaneous detection of several potential causative pathogens from a single specimen.
By consolidating diagnostic workflows, multiplex panels reduce the need for sequential testing and can play a central role in antimicrobial stewardship by limiting unnecessary antibiotic use1.
Challenges in Pathogen Differentiation: Rhinovirus vs. Enterovirus
One area of ongoing complexity is the differentiation between rhinoviruses and enteroviruses. Both belong to the family Picornaviridae and share high sequence homology, particularly in conserved regions of the viral genome targeted by many multiplex PCR assays2. As a result, many respiratory panels can only report a combined “rhinovirus/enterovirus” result, rather than distinguishing between the two.
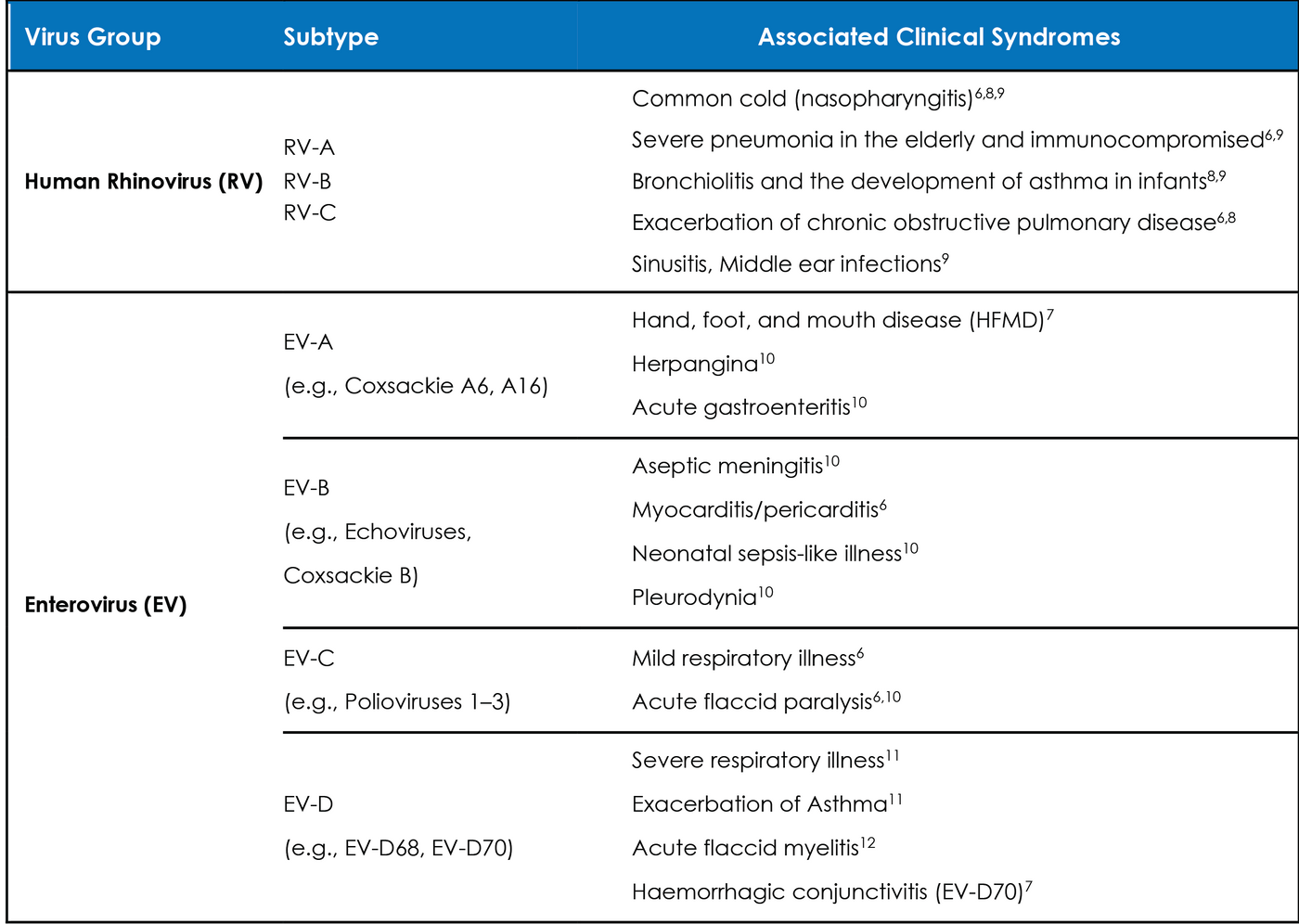
This limitation poses challenges for both clinicians and laboratory professionals. Table 1 summarizes common clinical syndromes associated with each. While rhinoviruses are the leading cause of the common cold and are typically associated with mild upper respiratory tract infections, they can also exacerbate asthma and chronic obstructive pulmonary disease (COPD)3. Conversely, enteroviruses are capable of causing a much broader spectrum of illness, ranging from respiratory disease to severe systemic infections, including aseptic meningitis, myocarditis, and hand-foot-and-mouth disease4. In particular, outbreaks of enterovirus D68 have been associated with severe respiratory illness and, in some cases, acute flaccid myelitis in children5.
Table 1: Human Rhinovirus (RV) and Enterovirus (EV) subtypes and their associated clinical syndromes.
The inability to reliably distinguish these pathogens on many panels can lead to diagnostic uncertainty. From a laboratory perspective, it raises interpretive challenges when communicating results to clinicians, who may need to consider additional clinical or epidemiological information to guide patient management.
Clinical Significance and Impact on Patient Care
The clinical implications of identifying specific respiratory pathogens are significant:
- Infection control: Prompt identification of influenza or RSV can lead to immediate cohorting and isolation, reducing nosocomial transmission13.
- Therapeutic decisions: Antiviral therapy for influenza, for example, is most effective when initiated early, underscoring the importance of rapid molecular detection.
- Risk stratification: Differentiating between mild rhinovirus infection and potentially severe enterovirus disease can impact patient monitoring and downstream testing (e.g., cerebrospinal fluid analysis if neurologic symptoms emerge).
- Public health surveillance: Accurate molecular diagnostics contribute to the recognition of viral outbreaks, supporting timely public health responses14.
Evolving Solutions
To address the challenge of rhinovirus-enterovirus differentiation, some molecular platforms are incorporating expanded genomic targets or reflex assays. Sequencing-based approaches offer definitive resolution but may be impractical for routine diagnostics due to cost and turnaround time15. As panel technologies evolve, balancing assay breadth with clinically meaningful discrimination will be critical. Laboratories may also consider reflex testing strategies when enterovirus outbreaks are suspected, ensuring that results are actionable for both clinicians and public health authorities.
For laboratory professionals, understanding both the strengths and limitations of current panels is essential for accurate result interpretation, effective communication with clinicians, and optimal patient care. Ongoing innovation in assay design will continue to enhance the utility of these powerful diagnostic tools in addressing the dynamic landscape of respiratory infections.
Interested in purely research applications for distinguishing between RV/EV, contact SpeeDx for a differentiating assay.
References
- Vidyasagar, V., et. al. (2023). Respiratory pathogen panels and antimicrobial stewardship: A narrative review. Journal of Antimicrobial Chemotherapy, 78(6), 1340–1349.
- Kumar, A., et. al. (2017). Challenges in the molecular detection of rhinoviruses and enteroviruses. Journal of Clinical Virology, 92, 25–30.
- Jacobs, S. E., Lamson, D. M., St. George, K., & Walsh, T. J. (2013). Human rhinoviruses. Clinical Microbiology Reviews, 26(1), 135–162.
- Tapparel, C., Siegrist, F., Petty, T. J., & Kaiser, L. (2013). Picornavirus and enterovirus diversity with associated human diseases. Infectious Genetics and Evolution, 14, 282–293.
- Messacar, K., et. al. (2018). Acute flaccid myelitis: A clinical review of US cases 2012–2015. Annals of Neurology, 83(5), 773–781.
- Royston, Tapparel. Viruses 2016 Jan 11;8(1):16
- Osterback et. al. J Clin Microbiol. 2013 Dec;51(12):3960-7
- Morelli et. al. Respir Res. 2025 Mar 28;26(1):120
- Rhinoviruses – U.S. Centres for Disease Control and Prevention. Available at: https://www.cdc.gov/rhinoviruses/about/index.html
- Xie et. al. Viruses. 2024 Jul 19;16(7):1165
- About Non-Polio Enteroviruses – U.S. Centres for Disease Control and Prevention. Available at: https://www.cdc.gov/non-polio-enterovirus/about/index.html
- About Enterovirus D68 - U.S. Centres for Disease Control and Prevention. Available at: https://www.cdc.gov/non-polio-enterovirus/about/about-enterovirusd68.html?CDC_AAref_Val=https://www.cdc.gov/non-polio-enterovirus/about/EV-D68.html
- Uyeki, T. M., et. al. (2019). Clinical practice guidelines by the Infectious Diseases Society of America: Seasonal influenza in adults and children. Clinical Infectious Diseases, 68(6), e1–e47.
- Centers for Disease Control and Prevention (CDC). (2020). Enterovirus D68 in the United States, 2020.
- Vogels, C. B., et. al. (2019). Multiplex PCR for routine respiratory virus surveillance. Clinical Infectious Diseases, 69(6), 940–948.