In the 21st century, oncology has achieved extraordinary progress. We can decode a tumor’s genome, tailor therapies to molecular targets, and extend survival through precision treatments. Yet, despite these advances, some patients still die not from cancer itself, but from the toxicity of drugs intended to cure them. There seems to be a gap between knowledge and practice everywhere. One of the clearest examples of this preventable harm is the overlooked DPYD gene test.
As clinicians know, the DPYD gene encodes dihydropyridine dehydrogenase (DPD), the key enzyme responsible for metabolizing fluoropyrimidine chemotherapy agents such as 5-fluorouracil (5-FU) and Capecitabine (Xeloda®). These drugs are commonly used to treat patients with colorectal/anal, pancreatic, breast, head and neck cancers [1].
In patients with partial or complete DPD deficiency, these agents can accumulate to toxic levels, leading to severe side effects including organ failure, life-threatening infections, and even death. Up to 8% of patients may carry DPYD reduced-function alleles. The death rate in the U.S. is estimated at 700 to 1,400 annually. A pre-treatment simple pharmacogenomic DPYD test can identify patients with DPD deficiency before treatment begins, allowing for safe, personalized dosing from the very first day of therapy [2,7].
Since 2020, the European Medicines Agency has recommended pre-screening and therapeutic dose management for Xeloda® (capecitabine) and warns of serious adverse reactions or death in patients with complete DPD deficiency [3].
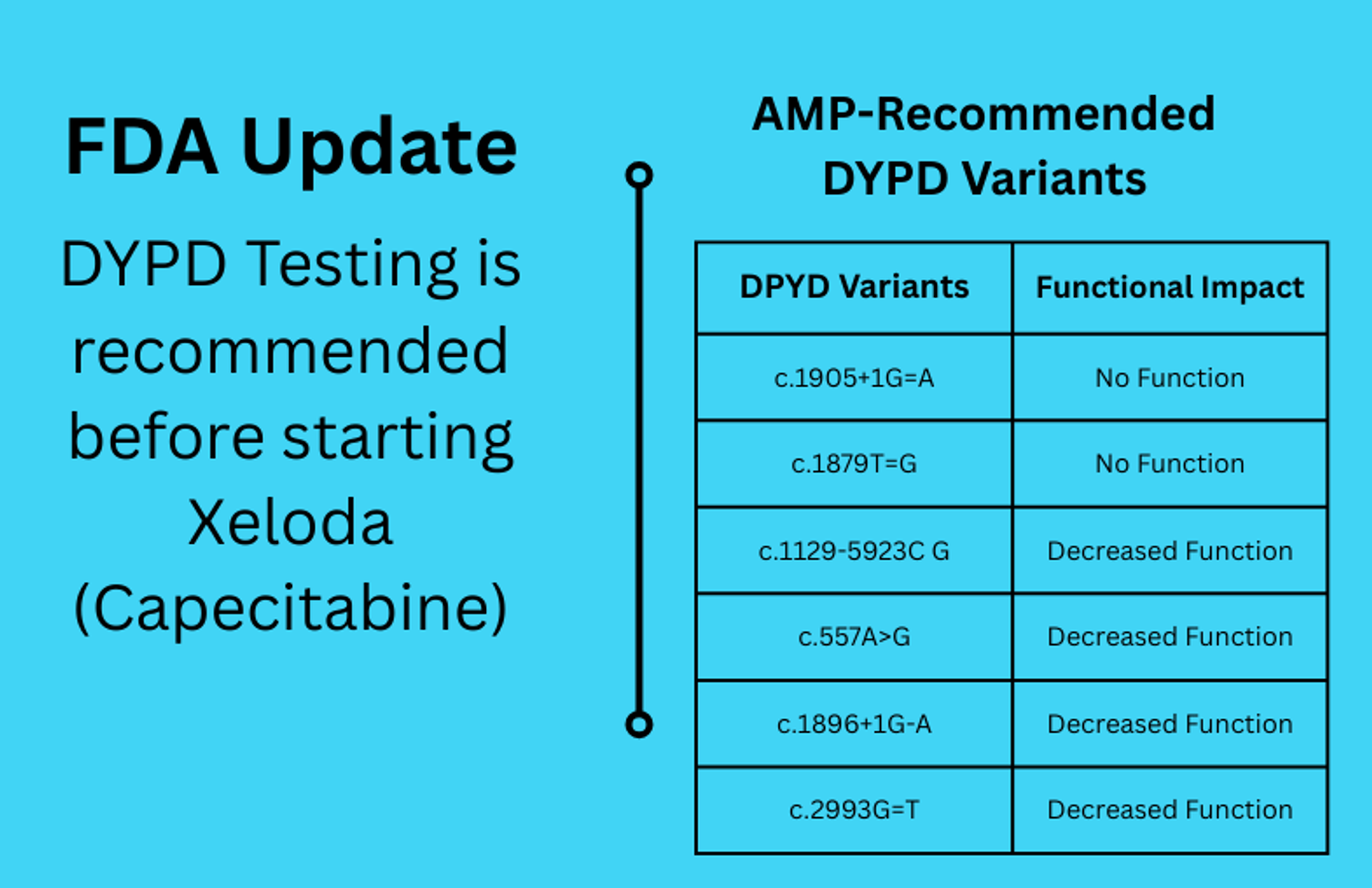 I am happy to say that the U.S. Food and Drug Administration (FDA) has recently updated the Xeloda® label to include a boxed warning recommending DPYD genetic testing before treatment [4,5].
I am happy to say that the U.S. Food and Drug Administration (FDA) has recently updated the Xeloda® label to include a boxed warning recommending DPYD genetic testing before treatment [4,5].
We also received more incredible news recently. On October 30, 2025, the National Comprehensive Cancer Network (NCCN) updated its guidelines for the treatment of colon cancer, requiring all cancer centers to perform DPYD testing before initiating chemotherapy. This landmark policy marks a decisive shift toward mandatory pharmacogenomic safety in oncology.
This is a major win for patient safety in the U.S., and we owe a dept to the tireless work of the Advocates for Universal DPD/DPYD Testing group, the entire pharmacogenetics society of US as well. Their work helped make this win possible, and their voices succeeded in turning science into policy [8,9].
Yet, in many oncology centers, the test is still not performed routinely, and when this crucial step is missed, the consequences can be catastrophic.
For a long time, clinical pharmacists and genetic laboratories have been alerted to the huge necessity of this test to prevent serious toxicity. The growing involvement of clinical pharmacists and genetic laboratories is transforming this landscape.
 I want to emphasize the crucial role of clinical pharmacists in translating pharmacogenomic results into therapeutic decisions, adjusting doses, choosing alternative regimens, and monitoring for toxicity. Their expertise bridges the gap between genetic data and bedside care, ensuring that treatment is both effective and safe. That’s why they are very well aware of this and see the adverse reaction of these medicines every day.
I want to emphasize the crucial role of clinical pharmacists in translating pharmacogenomic results into therapeutic decisions, adjusting doses, choosing alternative regimens, and monitoring for toxicity. Their expertise bridges the gap between genetic data and bedside care, ensuring that treatment is both effective and safe. That’s why they are very well aware of this and see the adverse reaction of these medicines every day.
As for genetic laboratories, they make every effort to equip themselves with advanced technologies and diagnostic tools, and development in technology, making many presentations for clinicians. But they must continuously monitor developments in genomics, including new protocols, clinically significant variants, and updated CPIC guidelines.
For example, the Association for Molecular Pathology (AMP) 2024 recommendations recently expanded the validated DPYD variant panel to include all 13 AMP-endorsed variants plus four additional ones (Tiers 1 and 2), with no added wells, workflow disruption, or material waste, even in resource-limited laboratories. Nevertheless, many clinical labs still use panel testing only for the four common variants, limiting diagnostic sensitivity. Clinical laboratories must explicitly report recent evidence (IJMS, August 2025) demonstrating incomplete linkage disequilibrium between the benign DPYD c.1236G>A variant and the pathogenic c.1129-5923C>G (HapB3) intronic variant. They have to avoid using c.1236G>A variant alone as a proxy marker check, and direct to test together with c.1129-5923C>G pathogenic variant [6,9].
Are all accredited laboratories following emerging evidence and variant interpretation? Are we sure about it?
Through close collaboration between genetic laboratories, clinical pharmacists, and oncology teams, real-time and individualized treatment planning becomes feasible and lifesaving.
Opinion: From Recommendation to Responsibility
Each of us must follow developments to see how significant the implementation of the DPYD test will be for oncologists after the FDA approved of its necessity.
We have knowledge, tools, and scientific expertise.
Now, we must commit to treating without harm and to ensure that precision medicine truly means personalized medicine.
Failure to perform DPYD testing prior to fluoropyrimidine administration is no longer a minor omission; it represents a systemic lapse in patient safety. In an era defined by precision medicine, neglecting available pharmacogenomic tools is unacceptable.
Every patient deserves a treatment plan designed not only for their cancer’s molecular profile but also for how their body metabolizes medication.
DPYD pharmacogenomics testing is not optional - it is essential.
Testing alone often isn’t enough. Doctors need a fast turnaround and an improved variant-inclusive solution. Let’s advocate for routine DPYD screening in every oncology center. It is a simple test, but a lifesaving one.
This Op-Ed is Published by Labroots in Partnership with the American Pharmacogenomics Association.
References
- Caudle, K.E. Thorn, C.F. Klein, T.E. Clinical Pharmacogenetics Implementation Consortium guidelines for dihydropyridine dehydrogenase genotype and fluoropyrimidine dosing. Clin Pharmacol Ther. 2013; 94:640-645.
- Sharma, B.B. Rai, K. Blunt, H. Pathogenic DPYD variants and treatment-related mortality in patients receiving fluoropyrimidine chemotherapy: a systematic review and meta-analysis. Oncologist. 2021; 26,1008-1016.
- EMA recommendations on DPD testing prior to treatment with fluorouracil, capecitabine, tegafur and flucytosine, 2020. EMA/229267/2020.
- FDA Black Box Warming https://lnkd.in/e6SDqE2e․
- ClinPGx (2025). Updated FDA-approved label for Xeloda (capecitabine), https://blog.clinpgx.org/updated-fda-approved-label-for-capecitabine/
- Victoria M. Pratt, Larisa H. Cavallari, Makenzie L. Fulmer, Andrea Gaedigk, Houda Hachad, Yuan Ji. DPYD genotyping recommendations, The Journal of Molecular Diagnostics, 2024; Vol. 26:10, 851-863.
- Jatta Saarenheimo, Hugo Willför, Nesna Wahid, Antti Jekunen, Heidi Andersén.. Impact of Upfront DPYD Genotyping on Fluoropyrimidine Adjuvant Therapy in Colorectal Cancer: A Real-World Data. 2025, Vol. 24: 2, 264-271.
- Gaedigk A., Casey S.T., Whirl-Carrillo M. Pharmacogene Variation Consortium: A Global Resource and Repository for Pharmacogene Variation. Clin. Pharmacol. Ther. 2021; 110:542-545
- Landrum M.J., Chitipiralla S., Kaur K. ClinVar: updates to support classifications of both germline and somatic variants. Nucleic Acids Res. 2025; 53:1313-1321.

![WGS for rare disease diagnosis [eBook]](https://d3bkbkx82g74b8.cloudfront.net/eyJidWNrZXQiOiJsYWJyb290cy1pbWFnZXMiLCJrZXkiOiJjb250ZW50X2FydGljbGVfcHJvZmlsZV9pbWFnZV84MmRlM2UyYjA5M2Q3ZTYwOTI3Zjc1YTRjOWU2N2RmMjkzMThjMTJkXzI1MDcucG5nIiwiZWRpdHMiOnsidG9Gb3JtYXQiOiJqcGciLCJyZXNpemUiOnsid2lkdGgiOjcwMCwiaGVpZ2h0IjozNTAsImZpdCI6ImNvdmVyIiwicG9zaXRpb24iOiJjZW50ZXIiLCJiYWNrZ3JvdW5kIjoiI2ZmZiJ9LCJmbGF0dGVuIjp7ImJhY2tncm91bmQiOiIjZmZmIn19fQ==)