Sarcoidosis is characterized by an exaggerated immune response to an unrecognized antigen, which has not yet been identified. It is an inflammatory disease of unknown etiology that presents with non-caseating granulomas, which are collections of macrophages that have attempted to wall off a foreign particle but have not been successful. Non-caseating means that there is no necrosis seen in the middle of the granuloma.
While sarcoidosis can affect any organ system in the body, it is found in the lungs of 90% of people diagnosed. Many people do not know they have the disease until it is seen on a chest x-ray. It manifests as bilateral hilar and mediastinal lymphadenopathy, which, by itself, is not specific for sarcoidosis. These abnormalities can also be seen with tuberculosis and lymphoma making a biopsy of the enlarged node necessary to make a definitive diagnosis.
Sarcoidosis is more commonly found in women, especially those of African-American descent. In the U.S., the incidence in whites is 11 in 100,000 people and blacks, 34 in 100,000. The prevalence is ten times greater for African-Americans than whites, and they experience greater severity in symptoms and chronicity.
Pathophysiology
The pathophysiology of sarcoidosis is not well-understood, but the activation of CD4+ T-lymphocytes (T-cells) is considered a hallmark indicator of the disease. A high CD4+/CD8+ ratio obtained from a bronchoalveolar lavage is another manifestation of sarcoidosis. Although there are large numbers of T-cells found in granulomas, many patients are reported to have significant lymphopenia (decreased blood lymphocyte levels) involving CD4, CD8, and CD19 T-cells. In addition to T-cell involvement, some biochemical levels have been found to be elevated including cytokines (interferon), tumor necrosis factor (TNF) and its receptors, and soluble HLA class I antigens.
Etiology
Even though there is evidence of physical changes within the body, the etiology of sarcoidosis is still unknown. Recent research has been directed at finding an infectious cause of granuloma formation. Two organisms that have been focused on are Propionibacterium acnes and Mycobacterium tuberculosis. P. acnes is an anaerobic gram-positive rod found abundantly on the skin and sebaceous glands and is implicated as a cause of acne. Its involvement in infections is controversial, and it has been found as a contaminant in tissue and surgical specimens. Recent studies have detected P. acnes in sarcoid cells (78%) through culture; however, Suzuki et al. wanted to determine if there were insoluble immune complexes (IICs) formed against P. acnes within the lymph nodes of sarcoidosis patients. IICs contain strongly antigenic and non-degradable substances that include microorganisms. They analyzed lymph node specimens embedded in paraffin and formalin-fixed from 38 sarcoidosis patients and 90 patients negative for sarcoidosis. An immunohistochemistry technique was utilized with anti-immunoglobulins (IgG, IgA, and IgM) and complement antibodies along with a P. acnes-specific monoclonal antibody. The authors found an abundance of P. acnes IICs within sarcoid lymph nodes and concluded that there might be an etiological link between the bacteria and sarcoidosis.
Management and Treatment
Many patients do not need treatment, and approximately 1/3 of people diagnosed will have complete resolution of their disease without requiring further intervention. Although there are no curative treatments available for sarcoidosis, medications used to manage it depend on the organ system affected. As with the initiation of any drug therapy, the potential benefits and risks have to be weighed. The two major factors that drive the necessity for treatment are if the symptoms are affecting activities of daily living and if the function of the organ is affected. Corticosteroids are the mainstay of medications used to treat symptomatic sarcoidosis. These drugs have side effects (increase in blood pressure, diabetes, edema, palpitations, insomnia, and mood changes) that some people cannot tolerate and alternative therapies have to be utilized. These can include the disease-modifying antirheumatic drug (DMARD) methotrexate, the antimalarial Plaquenil, the immunosuppressants azathioprine, cyclophosphamide, and Cellcept, and the TNF-alpha antagonists Remicade and Rituximab. Since sarcoidosis is due to an excessive immune response by the body, all of these drugs suppress the immune system and significantly increase the risk of developing a severe infection.
Severe and Opportunistic Infections
The risk of developing an acute, fatal infection in sarcoidosis patients is rare, but clinicians need to be aware of the presentation of symptoms and the need for an early diagnosis to prevent the occurrence of mortality and other sequelae.
Pneumocystis jirovecii (PCP)
Pneumocystis jirovecii (PCP) is a yeast-like fungus that can cause severe, life-threatening pneumonia in immunocompromised people. It is rare to see it in a healthy person. When it was first seen in HIV patients in the 1980s, it was termed Pneumocystis carinii and was thought to be a protozoan parasite. It was reclassified in 2001 as a fungus based on the fact that its cell wall composition is more closely related to a fungus than a protozoan.
PCP has long been an AIDS-defining illness in those infected by HIV; however, due to the utilization of high-activity antiretrovirals and standard prophylaxis, PCP infections in HIV patients have significantly decreased. At the same time, PCP has emerged as a pathogen in people who have non-HIV-related immunosuppression due to drugs that are immune-suppressive. Prophylaxis for PCP is common in HIV patients but not so much in sarcoidosis. Fahim in the Journal of Clinical Outcomes states that routine prophylaxis with trimethoprim-sulfamethoxazole needs to be discussed with the patient in the following situations:
- a corticosteroid dose of greater than 20 mg per day
- the combined use of corticosteroids at greater than 20 mg per day and anti-TNF drugs
- presence of sarcoidosis and a comorbid condition that produces significant immune suppression
Although a diagnosis of PCP is usually first made by the patient's symptoms and chest imaging, confirmatory testing includes the demonstration of the yeast through staining or PCR testing of induced sputum or bronchoalveolar lavage.
Cryptococcus neoformans
Cryptococcus neoformans is another opportunistic infection seen due to immunosuppression in sarcoidosis. C. neoformans is an encapsulated yeast frequently found in cerebrospinal fluid in patients with meningoencephalitis. In sarcoidosis, recognition of possible infection by this organism can be delayed when the clinician is considering neurosarcoidosis as a diagnosis. C. neoformans has also been correlated with HIV in the past, but because of prophylaxis, it is being seen more in non-HIV immunosuppressed patients. Delayed diagnosis is associated with poor outcomes and increased mortality.
Cryptococcosis can be identified through culture with gram stain and cryptococcal antigen on blood and CSF. The presence of encapsulated yeast can also be seen by performing a wet prep exam with India ink.
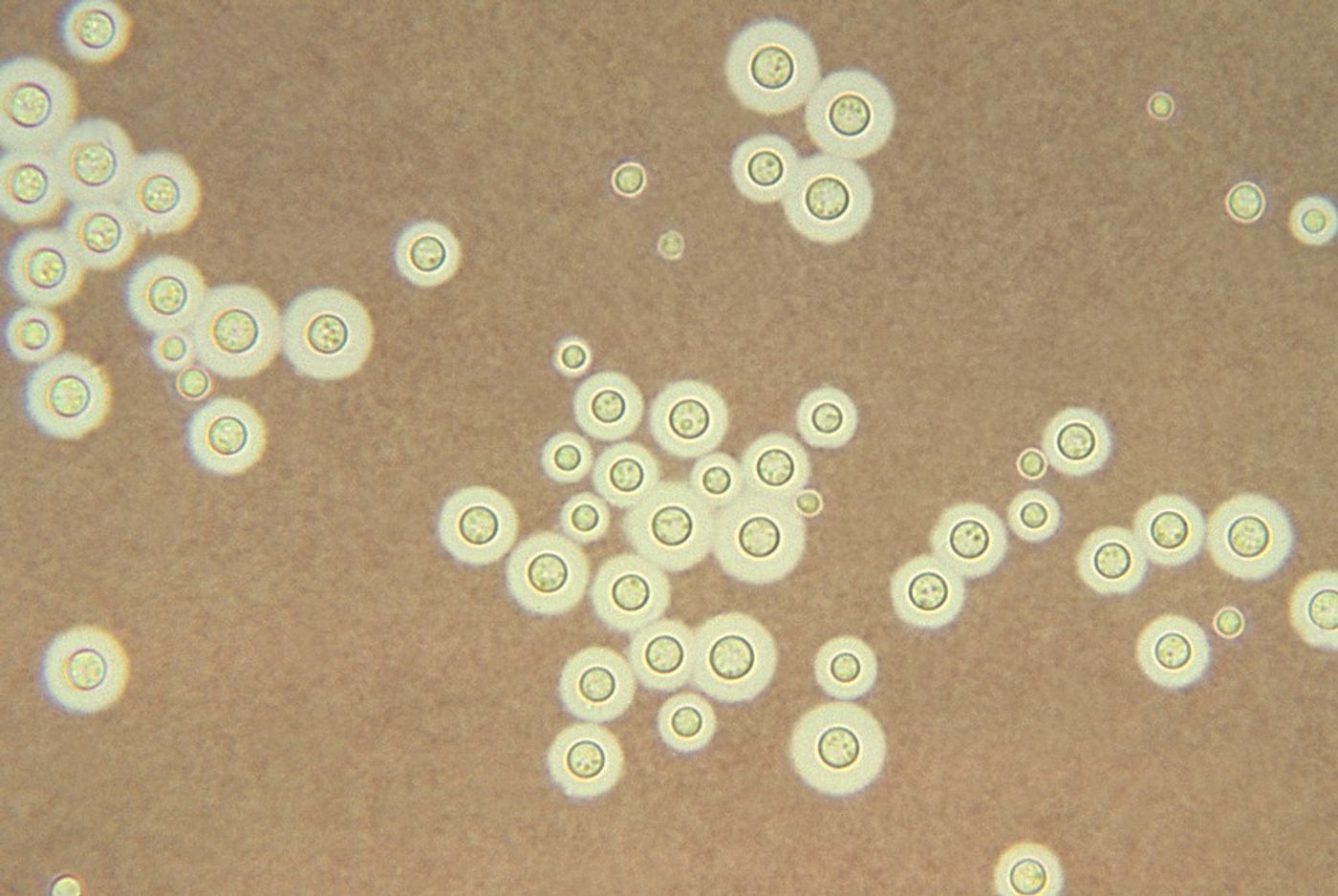
Encapsulated C. neoformans in India ink prep.
(Credit to Centers for Disease Control and Preventions Public Health Image Library (PHIL)
Laboratory diagnosis of C. neoformans is essential for this type of infection. The India ink exam is a quick test that can reveal cryptococcosis in CSF, but it has a very low sensitivity and can miss low numbers of the yeast. While the gold standard is culture, it is time-consuming and may take a couple of days to grow. Serological tests include latex agglutination and ELISA assays, and the immunochromatography test, lateral flow assays, have greater than 90% sensitivity and can detect C. neoformans in asymptomatic patients.
Opportunistic infections by almost any organism can be seen in a person who is severely immune suppressed. A quick review of the literature revealed rare infections including fungi (T. marneffei, Aspergillus, C. albicans), mycobacterial infections (MTB), bacteria (Pseudomonas, E. coli, Haemophilus influenza), viruses (CMV, HHV-8), and parasites (Strongyloides stercoralis ).
Dureault et al., when considering age, ethnicity, sex, and corticosteroid use, identified two major predictors of severe infection: treatment and affected site. Treatment with three or more immunosuppressants or cyclophosphamide or localization in the heart or nervous system were associated with a high risk for severe infections.
Even though severe infection is not common in sarcoidosis, clinicians need to be aware of factors that can lead to an opportunistic infection. As is true for any disease, early recognition of the signs and symptoms of infection allows for initiation of aggressive treatment that can save the patient's life. However, in infections such as C. neoformans and PCP, there is still a high rate of mortality even with treatment. Prophylaxis for these two microorganisms is standard in HIV patients and is crucial for sarcoid patients who meet specific conditions. As advances are made in the understanding of the etiology and pathophysiology of sarcoidosis, the possibility for new treatments that do not increase the risk of severe infections exist.