Background
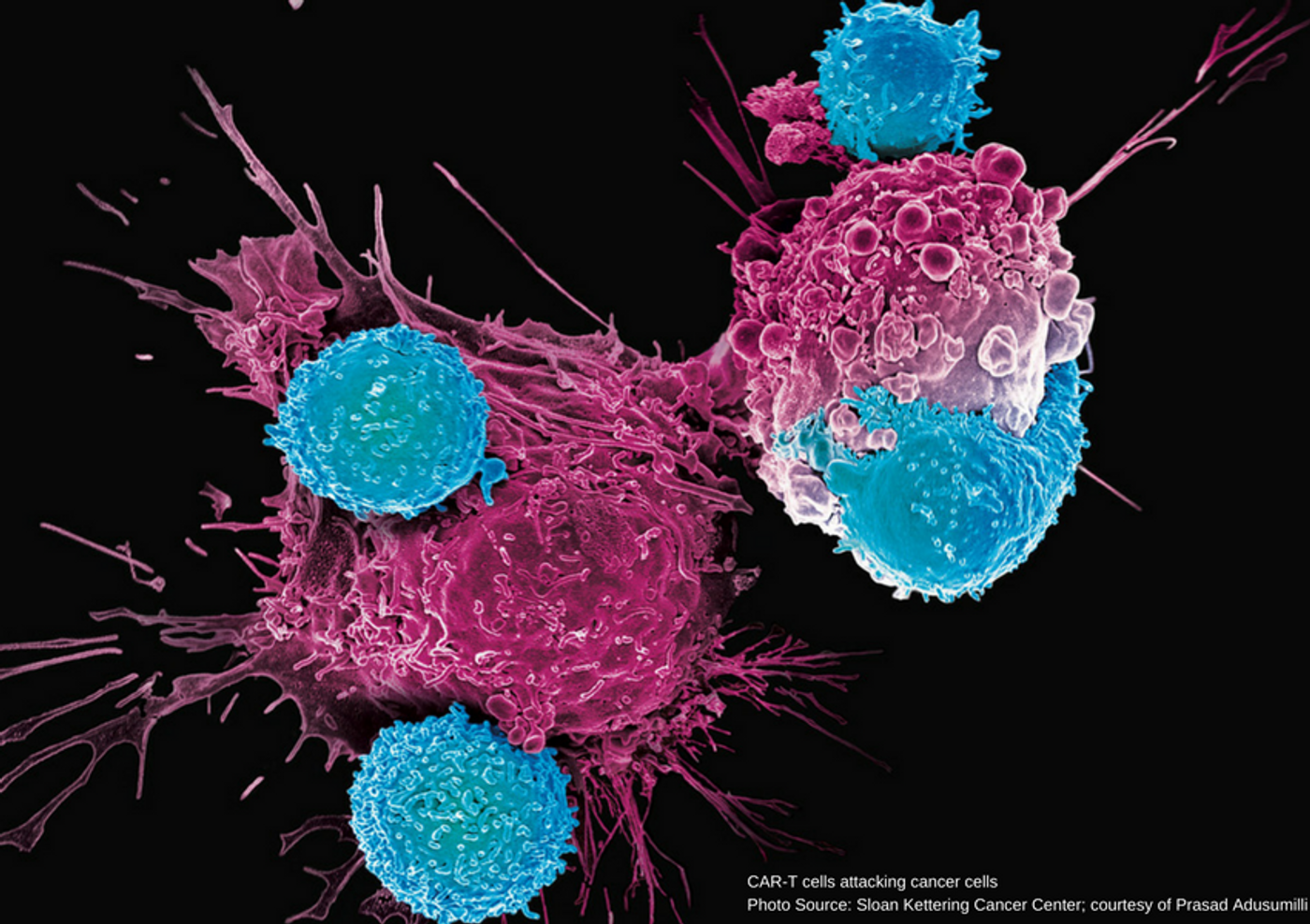
Over the past few decades, cancer therapies have included the “four pillars” of treatment including surgery, chemotherapy, radiation therapy, and targeted drug therapies against cellular changes in certain cancer cells such as imatinib (Gleevec®) and trastuzumab (Herceptin®). Some in the cancer community have called immune-oncology, or immunotherapy, the potential “fifth pillar” of cancer treatment. Immunotherapy approaches are currently focused on adoptive cell transfer (ACT); the patient’s own cells are collected and manipulated to be used to treat that patient’s cancer. There are several types of ACT including tumor infiltrating lymphocytes (TILs), endogenous T-cell therapy, chimeric antigen receptor T cells (CAR-T cells), and T cell receptor transduced cells (TCR). Research is being conducted on each of these types; however, the most successful therapy, and the one gaining immense traction, is CAR-T cell therapy. Two CAR-T cell therapies were approved by the FDA in 2017, one for childhood acute lymphoblastic leukemia (ALL) and the other for adult advanced lymphoma; both cancers are B cell malignancies.
CAR-T cells, and ACTs in general, are distinct because they blend the theory of the earlier generation of targeted drugs from the late 90’s, like Gleevec®, and the incredible abilities of an individual’s immune system. One challenge with therapies that use cells from others is the potential for rejection due to incompatibility. CAR-T cell development is a brilliant development that eliminates that general incompatibility risk factor; in addition, technological advances have provided researchers the opportunity to hypothesize, actually create, and implement the use of these successfully for a small handful of cancers.
CAR-T Cell Preparation
The initial steps include leukapheresis where T-cells are separated, and the remaining blood volume returned to the patient. T-cells are further filtered to provide CD4/CD8+ cells for subsequent steps. The separated T-cells are transfected using a viral vector containing the chimeric antigen receptor (CAR) gene to force the T-cells to express CAR on their surface. The newly approved CAR-T cells for ALL and adult lymphomas recognize CD19 on the cancerous B cells contributing to disease. The viral vector is in the form of RNA which, when introduced to the cells, is reverse-transcribed in the nucleus and integrated into the cellular DNA. Those cells are then pushed to begin replicating and dividing so that continued expression and cell duplication, with the CAR, is maintained. Of note, at the start of research and development of this expansion process, it took up to a few weeks to produce enough CAR-T cells to use for infusion; nowadays, many labs have honed the process and reduced that time to less than 7 days. Once the cell expansion process is completed, often resulting in 5 liters of cells in culture, the cell culture is concentrated and cryopreserved in an infusible medium to be delivered to the institution where the patient will be treated and then infused.
Patient Preparation
Somewhat similar to a bone marrow transplant (BMT), or hematopoetic stem cell transplant (HSCT), the patient is prepared for CAR-T cell infusion with a chemotherapy regimen. The purpose of this is lymphodepletion. As with any treatment that reduces a patient’s immunity, a high degree of monitoring takes place to reduce any chances for infection. When providers determine the patient has been sufficiently prepared, the CAR-T cells are infused.
Risks
CAR-T cell therapy is not without risks. One risk that can develop early on is cytokine release syndrome (CRS) in which the normal process of T cell cytokine release is expanded due to the increased T cell load. CRS results in substantial release of cytokines into the bloodstream which can give rise to high fever and unexpected drops in blood pressure. In thinking about the physiological process occurring, CRS or similar symptoms, are a positive indicator that the CAR-T cells are actively working. Time and experience have helped providers and researchers prepare for successful management of CRS when it does occur.
Future
CAR-T cell therapies show incredible promise for treatment of cancer using the patient’s own cells. These therapies are of great interest because they are potentials for treating cancers that are refractory. Patients that had exhausted all other options were the initial clinical trial participants and, in the cases of the two approved therapies mentioned previously, the long-term response rates promoted CAR-T cell therapy into the forefront of the oncological stage. There is still much to be done to investigate further uses and potentials of CAR-T cell therapies, but advances are being made daily, in research and in the ability to produce CAR-T cells for patient treatments. The potential is there for expansion of this therapy, though some are not sure that this will prove a viable option for solid tumor disease treatment. Additional research on other clusters of differentiation are being investigated including CD22, CD70, CD20 and more.
Sources: NIH National Cancer Institute, Molecular Therapy-Methods & Clinical Development Journal, FDA, American Society of Hematology, Journal of Clinical Oncology, Melanoma Research Alliance, Neurology Oncology,